

Number37
Anyhow, have a Winfield 25.
- Oct 5, 2013
- 22,222
- 24,270
- AFL Club
- Sydney
yeah, that's why you drink water. 250ml per hour if lounging, 500ml if dancing. oh no won't somebody think of the children!?
all avoidable by the responsible user with the right amino acid.
well, in an informal sense i use "safe" to mean you don't OD or die from taking mdma. i realise you'll have some ignorant media example in contrast, but in reality mdma deaths are mostly caused by alcohol, substances that aren't mdma, or people who can't manage the 250/500 water rule. there are innumerable prescription drugs that are more dangerous or require more management.
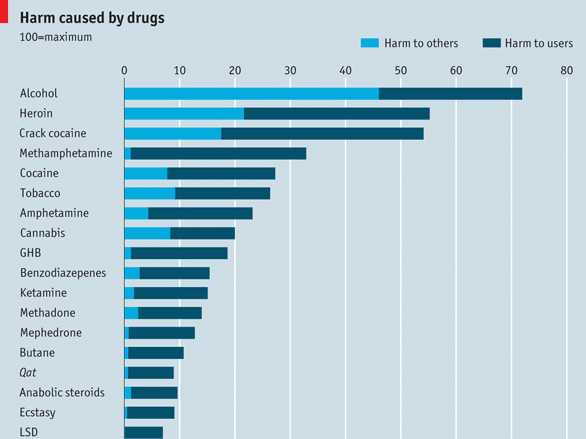
ive referenced the lancet study before, but here it is again. mdma almost last.

eta- i mean do we really have to bring out all the studies about how dangerous bacon, sitting down, or using the internet is? life is a risk.
It doesn't look like a lot but how many of those 'others' is someone minding their own business?
That alcohol stat is something we should all have a good think about!
